PHS Launches Task Force to Address PCP Shortage
Michael Lambert, MD, routinely discusses career choices with residents as they begin to decide between practicing general medicine as a primary care physician or in a specialty, like cardiology.When running down the pros and cons of being a PCP, Lambert has no trouble listing many positive attributes of enjoying long-term relationships with patients, diagnosing and treating a wide range of diseases and conditions each day and working with patients to resolve those issues over a long period of time.
“But primary care is losing out,” said Lambert, a primary care physician who has practiced at Southern Jamaica Plain Health Center for more than 20 years.
With graduating medical students facing as much as $200,000 in college loans to repay, financial remuneration is one of the most pressing reasons that health care is facing a shortage of primary care physicians. With the Massachusetts Health Care Reform Act now requiring all residents to have health insurance, the demand for PCP services is expected to increase even more.
To counteract this alarming trend, Partners HealthCare in July launched the PHS Primary Care Task Force to develop a strategy for primary care focusing on adult internal medicine to ensure the quality of care is superior and appropriate and can be realistically offered to patients. In addition, the task force will examine recruitment and retention issues such as job structure, work-life balance, career development, compensation and workflow issues.
“It’s clear we need to do something, and we’re moving forward with great energy and support,” said Robert Goldszer, MD, MBA, BWH’s associate chief medical officer and director of Primary Care, who co-chairs the task force with Brit Nicholson, MD, chief medical officer and senior vice president for Primary Care Administration at MGH.
PCP Shortage, Increased Demand Could Equal Crisis
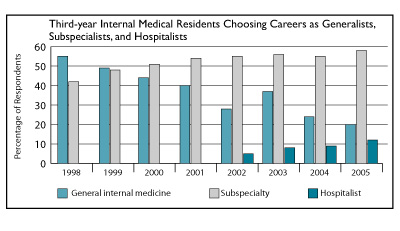
In recent years, many national media outlets and health care organizations have called the shortage of primary care physicians a crisis. In 2006, the American College of Physicians warned that “primary care, the backbone of the nation’s health care system, is at grave risk of collapse.” Fewer PCPs are entering the profession, with many physicians instead opting for careers as specialists. PCPs are taking care of more patients who are getting older and sicker and who require a more complex array of preventive, diagnostic and treatment options. In addition, many PCPs are reducing their hours and the number of patients they see.
And the demand for PCPs is expected to increase significantly in the next year, especially as the Massachusetts Health Care Reform Act is implemented. The new state law requires all residents to have insurance, and this will increase the demand on patients to see their PCP.
“As everyone tries to make the health care system better, it becomes a lot harder on the primary care physician,” said Brad Weiner, MD, who practices at BWH Primary Care Associates of Brookline.
Challenging but Rewarding
Like Lambert, Weiner stresses the positive aspects of being a primary care physician. “PCPs develop very long-lasting and meaningful relationships with their patients, often times also caring for their patients’ spouses, siblings, parents and children,” he said. “This, combined with the opportunity to treat a wide variety of illnesses and conditions, develop unique relationships with specialists and engage in continual learning, makes it a very rewarding career.”
But the perceived negatives associated with being a PCP, such as high volume of patient visits and compliance and paperwork demands, have gained more traction in the health care industry, say Weiner and Lambert. A typical day for a PCP would start at 7 a.m. to review lab results, return phone calls and e-mails and communicate with specialists. The patient visits start at 7:30 a.m., and many PCPs see a patient every 15 minutes all day long.
“The PCP books 32 hours a week, sees patients for 15 minutes, and seeing a new patient or a physical exam can last 30 minutes, and many of us have to book extra patient visits to account for the people who don’t show up or cancel,” Lambert said.
Four hours of patient visits typically result in two hours of paperwork, he added. “It can be a very busy day, often times with a working lunch,” he said.
While both Lambert and Weiner know their cardiologist counterparts and other specialists are just as busy, primary care physicians traditionally earn less income.
“It’s not just the salary,” Weiner said. “Loan debt is really affecting the career choice of young physicians.” When Weiner graduated from medical school seven years ago, many of his classmates faced $160,000 in school loans, and now medical school debt is approaching $200,000.
“The cost of living in the greater Boston area is significantly higher when compared to the surrounding communities, and this now influences where physicians choose to practice medicine,” he said.
Addressing the Issue
One recent development, which Weiner calls a “great step in the right direction,” is a loan repayment program sponsored by PHS, Bank of America and the state of Massachusetts to provide PCPs assistance to repay loans in return for practicing in a city community health center. In addition, PHS, BWH and MGH have increased starting salaries for PCPs and added clinical support in new physician assistants, pharmacists, social workers and administrators.
The primary care task force plans to survey all PHS PCPs. The group also formed four separate subcommittees. One will examine practice models and job descriptions. There is a subcommittee on mentorship and career satisfaction, as well as a group charged with scrutinizing compensation models. Lastly, a subcommittee will examine health and public policy issues with a regional and national perspective.
“Primary care is a very rewarding field, but it is not in a great place right now,” said Weiner. “But it remains a very important position in the way we deliver quality care, and it’s a very attractive career choice, one I certainly would not change.”